
Baby carriers are very easy to handle, however, quality varies between manufacturers so you should choose carefully. The most important considerations are correct leg position, sufficient back support, and stabilization of the head.
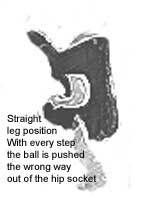
You should first check the leg position of your baby; most baby carriers do not ensure the correct positioning. Some carriers have openings where the baby’s thighs hang almost straight down. This design does not provide adequate support. In some cases, a squatting leg position is not only impossible, but in the face-to-face orientation, the thighs and knees of the child are pressed up against the adult. With each step of the baby wearer, the child’s knees are pushed backward. When this happens, the additional pressure from the child’s thighs increases the amount of stretching on his or her hip joints.
When looking at tube slings or ring slings, watch for slings that are too short. The entire bottom of the sling, even when used with a four month old infant, hardly reaches up underneath the shoulder blades. With most of these slings, the suggested age is 3-4 months, however, even at that age these types of slings do not stabilize the back and shoulders sufficiently. Although these carriers seem practical, they simply do not offer your baby sufficient support, especially on prolonged walks.
Explaining Hip Dysplasia
The femur (thighbone) is the longest and strongest bone in the body. Proximally, the femur has the following: head which fits in the acetabulum of the coxal bone (hip socket) greater and lesser trochanters which provide a place of attachment for the muscles of the legs and buttocks; linea aspera, a crest that serves as a place of attachment for several muscles.
Ball-and-Socket Joints
In the ball and socket joints, the ball-shaped head of one bone fits into the cup-shaped socket of another. Movement in all planes is possible, as well as rotation. The shoulder joint and hip joint are examples of this type.
Hip Dysplasia can be either congenital (CHD) or developmental (DDH) and occurs when the top of the femur (leg bone) is not properly located in the hip socket or not located where the hip socket is expected to develop. Hip dysplasia in humans is normally diagnosed in babies. Statistically, girls have a higher incidence of hip dysplasia than boys. There are a variety of treatments that are used depending on the age of the child and the severity of condition.